


For many women, irregular periods are one of the first signs that perimenopause has entered the chat. Most of the time, a heavier flow, midcycle spotting, and unpredictable bleeding are the result of midlife hormone shifts and, while inconvenient and annoying, are perfectly normal. At other times, they may hint at underlying issues, such as thyroid problems or fibroids. Regardless, if you’re in your 40s or early 50s and your period has started acting up, relief is available. Midi Health has the straightforward, hormone-smart guidance you need to understand if and when to worry about perimenopausal bleeding, including whether it’s time to seek help.
When it comes to adulting, knowing when to worry about perimenopausal periods ranks right up there with paying taxes and scheduling your first colonoscopy. It’s not fun, but it’s important.
Because the truth is that when you’re in the 4- to 10-year march toward menopause, your menstrual cycle will enter its IDGAF era. One month, your period might show up annoyingly early, like a party guest ringing your doorbell while you’re still doing your makeup. Then it might go MIA for a few months, only to pop up when you least expect it…and with flash-flood energy, at that.
“For many women, shortening of cycles is one of the first signs of perimenopause,” says ob/gyn Mindy Goldman, MD, Midi’s Chief Clinical Officer. “Instead of every 28 to 32 days, you might get your period every 24 to 26 days. In the later part of perimenopause, people tend to skip cycles, or it may stretch out and be more like an every-40-day cycle.”
When researchers reviewed the menstrual cycles of 51,000-plus women ages 42 to 52 who participated in the Study of Women's Health Across the Nation (SWAN), they learned that most experienced multiple periods lasting a week or more. Perimenopausal spotting for 6 or more days was common, too.
All of this period drama isn’t just annoying; it can leave you feeling anxious, overwhelmed, or even scared. (No one feels peaceful while Googling, “Why am I spotting 2 weeks after my last period?”)
If unpredictable perimenopause bleeding has you seeing red, you’ve come to the right place.
Perimenopause Bleeding Basics: What’s Normal vs. What’s Not
Before perimenopause, your estrogen and progesterone levels likely stuck to a predictable pattern. About every 28 to 32 days, those hormones work in harmony, telling the uterus: “Time to let that lining go.” The result: your monthly period.
Throughout the menopausal transition, your estrogen levels decline, but with lots of spikes and dips along the way. (Progesterone declines, too, but not as erratically.) Considering that period regulation is one of E and P’s main roles during your reproductive years, it’s not necessarily surprising that as those levels go wonky, so do your periods.

No two women are alike, but in general, the most common changes include heavier bleeding, less predictable cycles, midcycle spotting, and worsened PMS symptoms.
“If you have questions about your bleeding pattern, it’s important to talk to your clinician,” Dr. Goldman says. “Cycle change is very, very common in midlife, but frequent irregular bleeding warrants an evaluation.”
Perimenopausal period puzzler #1: Heavier periods (and sometimes clots)
Irregular ovulation during perimenopause can lead to fluctuating estrogen levels. That, combined with less progesterone (which helps stabilize the uterine lining, Dr. Goldman explains), can allow the uterine lining to build up excessively. The thicker the lining, the heavier the period. You may pass jelly-like clots, too.
As one perimenopausal UK woman put it when interviewed by researchers for a 2023 paper about perimenopause and well-being: “Then perimenopause kicked in…I didn't actually realise what was happening, but every few months I would have an incident where I literally flooded. I did it in restaurants. I did it on buses, and you know, when you were just like ‘[T]hat's not even possible,’ the sheer amount of blood…”
Perimenopausal period puzzler #2: Spotting or lighter periods
“Women will ask me, ‘Why am I spotting 2 weeks after my last period?’” Dr. Goldman says. The answer: The unpredictable rise and fall of perimenopausal estrogen and progesterone levels can send mixed signals to your reproductive system about when it’s time to shed its uterine lining. In response, your uterus may shed part of its lining during non-period hours. Period panties are your friend.
What causes spotting is similar to what can cause lighter periods: As estrogen levels fluctuate in perimenopause, especially early perimenopause, your periods can become lighter or seem more like spotting than an actual flow.
Perimenopausal period puzzler #3: Less predictable cycles or missed periods
During early perimenopause, short cycles (fewer than 21 days) are common. In later perimenopause, cycles start to space out, growing longer (more than 36 days apart). You may miss a cycle every once in a while, maybe even several in a row, especially as you inch closer and closer to menopause, when cycles stop completely.
“To have normal, regular menses, everything has to be in sync,” Dr. Goldman says. “During perimenopause, the brain and ovaries get out of sync, hormone levels can fluctuate, and it’s very common that women don’t ovulate on a regular basis. People can have less predictable cycles, and they can miss periods entirely.” These fun little games of hide-and-seek frequently end with an out-of-nowhere period, aka a “flash period,” as made famous by a white jumpsuit-clad Charlotte on And Just Like ThatAnd Just Like That.

Perimenopausal period puzzler #4: Worsened PMS symptoms
This one isn’t related to the bleeding aspect of periods, but rather to the overall perimenopausal period experience. Technically speaking, the light at the end of the perimenopausal tunnel is the end of PMS symptoms like monthly breast tenderness, bloating, and mood shifts. However, those symptoms may worsen before they improve. In recent research published in Post Reproductive Health, women approaching menopause described worsened breast tenderness, headaches, mood swings, and other PMS symptoms, compared with their earlier reproductive years.
Estrogen and progesterone are involved in plenty of other bodily processes, too, which is why changing levels during perimenopause can lead to non-period-related symptoms, such as hot flashes, insomnia, mood changes, brain fog, weight gain, and more.
To be fair, this isn’t all estrogen’s fault. Stress, diet, weight gain, and other lifestyle factors can impact your cycle. For instance, in a review of 41 studies involving nearly 40,000 women from 30 countries, a variety of stressors—including occupational stress, academic stress, and COVID-19 pandemic stress—were linked with irregular periods, abnormal menstrual flow, and other menstrual disruptions.
Additionally, up to 30% of women worldwide who are of reproductive age experience abnormal bleeding (bleeding that’s unusually long, irregular, or heavy) linked to medical conditions, such as:
- polycystic ovary syndrome (PCOS), a common hormonal disorder that causes the ovaries to produce excess testosterone
- thyroid problems
- fibroids, which are benign tumors of the uterine muscle
- endometriosis, when cells similar to the uterine lining grow outside the uterus
- endometrial hyperplasia, when the lining of the uterus becomes too thick
- adenomyosis, when the endometrial tissue grows into the uterine muscle
- sexually transmitted infections (STIs)
- type 2 diabetes
- an out-of-place intrauterine device (IUD)
- certain types of cancer
How Abnormal Perimenopausal Bleeding Is Evaluated and Diagnosed
If you’re wondering when to worry about perimenopausal bleeding, the next step is an evaluation that looks for the cause of heavy, prolonged, or irregular bleeding—and rules out underlying conditions.
Bring a two-cycle bleeding tracker to your appointment. Record:
- how many pads or tampons you use per hour
- the size and number of blood clots
- symptoms such as fatigue, dizziness, pelvic pain, or shortness of breath
- missed pills, new medications, or other cycle disruptors
This data helps your clinician determine whether your perimenopause bleeding, perimenopause spotting, or bleeding for 3 weeks falls within the wide range of hormonal changes—or needs further testing.
Also bring a list of medications, birth control, and any personal or family history of fibroids, thyroid disease, or bleeding disorders.
Blood tests
Blood work checks for common medical causes of abnormal bleeding and complications from heavy flow.
- CBC and ferritin: Evaluate for iron-deficiency anemia caused by prolonged or heavy perimenopause bleeding, especially if you have fatigue, weakness, or shortness of breath.
- TSH (thyroid test): Thyroid disorders are a frequent and treatable cause of spotting and irregular cycles.
- Pregnancy test: Ovulation can still occur in perimenopause, which is why pregnancy must be ruled out.
Imaging
Transvaginal ultrasound is the first-line imaging test for abnormal uterine bleeding. It can detect:
- fibroids
- polyps
- a thickened uterine lining
- ovarian cysts
- adenomyosis
These structural conditions commonly contribute to heavy or unpredictable perimenopause bleeding.
Endometrial biopsy
This test samples the uterine lining to rule out endometrial hyperplasia or cancer. It’s typically recommended if you:
- are 45 or older
- have very heavy or prolonged bleeding that doesn't improe with initial treatment
- have risk factors, like a family history of uterine cancer
Pelvic exam
An in-person exam may be needed to assess the uterus and cervix and check for infection, polyps, or other visible causes of bleeding. (A Midi clinician can refer you to an ob/gyn if required.)
Treatment Options
According to a recent survey, 70% of women ages 40 to 65 were not currently receiving treatment for for symptoms during the menopause transition. But why suffer through tsunami periods or worry about spotting during your cycling class when so many real solutions for managing perimenopausal periods are out there? A clinician can help you craft a care plan featuring lifestyle changes, medical treatments, and natural remedies to bring you relief and help you feel more in control of your perimenopause experience.
Rx Solutions
Combined hormonal birth control—the types that use estrogen and progesterone—can help regulate periods and alleviate heavy menstrual bleeding and pain. Examples include oral contraceptives (“the pill”), patches, vaginal rings, and levonorgestrel IUDs such as Mirena or Kyleena. These IUDs release a progesterone-like synthetic hormone that “stabilizes the lining of the uterus, protecting it from getting too thick—many women don’t get their period at all” while using a hormonal IUD, Dr. Goldman says.
Speaking of IUDs, non-hormonal IUDs (like ParaGard and Miudella) don’t ease perimenopausal bleeding issues. In fact, they can cause heavier or longer periods.
As a bonus, hormonal birth control helps you avoid getting pregnant. Yes, you can still conceive in perimenopause, since you’re still ovulating. According to the American Society for Reproductive Medicine, by age 40, a sexually active woman’s odds of conceiving are less than 5% per cycle. Still, while chances of pregnancy decrease, 77% of pregnancies that occur in women in their 40s are unintended, and since periods are irregular, detection of pregnancy may be delayed.
Hormone Replacement Therapy (HRT)
Often referred to as menopause hormone therapy (MHT), HRT supplements estrogen and progesterone levels during perimenopause. This improves not only period symptoms, but other symptoms related to fluctuating hormone levels, including vasomotor symptoms like hot flashes, vaginal dryness, and mood shifts. HRT is available in many forms, including patches, pills, creams, and gels, and it should be tailored to your health history and symptoms.
HRT isn’t for everyone. Some women aren’t candidates, due to a history of stroke or certain types of blood clots; certain heart or liver problems; or hormone-sensitive cancer, including certain breast and uterine cancers. Your clinician can help you determine whether you’re a candidate.
Be forewarned that HRT is not a form of contraception. The doses used in perimenopause are “about ⅓ to ⅕ the dose of what’s in oral contraceptives,” Dr. Goldman says—not enough to suppress ovulation or protect against pregnancy.
Ironically, it’s common to experience spotting or heavier or more frequent bleeding in the first 1 to 3 months after starting HRT. These bleeding changes occur because HRT hormones can stimulate the uterine lining, causing it to shed as if it were a period. Usually, this is nothing to worry about, but it’s worth checking in with your doctor or Midi clinician a month or so after starting HRT. As your body adjusts to HRT, the bleeding should resolve. If not, your clinician may try adjusting your prescription.
Over-the-Counter Treatment Options
- If you can safely use nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, try taking them on your heaviest period days to ease blood flow and cramps. Tranexamic acid, a prescription medication used to treat heavy menstrual bleeding by promoting blood clotting, may also help. (Contraindications for tranexamic acid include active blood clots or certain heart conditions.)
- Heat therapy, such as a heating pad or warm bath, can relax muscles and soothe cramps.
- Heavy bleeding can deplete your iron stores, causing fatigue and low energy. Tell your clinician if you’ve been feeling unusually tired or lightheaded; they may want to check your iron levels. If you’re low, they may suggest adding iron-rich foods, such as leafy greens, eggs, red meat, and beans, or an iron supplement.
If your clinician determines that thyroid problems, fibroids, or another condition is behind your worrisome perimenopausal bleeding, they can explain different treatment options.
Lifestyle Treatments for Specific Conditions
Lifestyle boosts, such as a consistent exercise routine, balanced diet, and stress management, won’t directly impact perimenopausal bleeding or perimenopausal spotting. Still, they can help improve symptoms of PMS or other medical conditions. For instance:
- Regular physical activity can help ease the mood shifts and cognitive difficulties of PMS. Endorphins and other hormones released during exercise can also help ease cramps, bloating, and headaches by stimulating the body’s natural anti-inflammatory processes, per a 2024 Annals of Neuroscience review.
- If PCOS is driving your perimenopausal bleeding issues, eating in ways that improve insulin sensitivity may help. (Insulin resistance is linked to PCOS and high testosterone levels in women.) Limiting sugary and processed foods and prioritizing low glycemic-index foods, for instance, has been linked with more regular menstrual cycles in women with PCOS.
- Living with abnormal uterine bleeding can take a toll on your mental health; anxiety and depression are common in perimenopausal women who find themselves constantly stressing about how long or heavy their period is or wondering when it will hit. A 2025 BMC Psychology study concluded that lifestyle interventions such as exercising more, improving sleep, and quitting smoking “may offer substantial benefits in alleviating psychological distress during this vulnerable period.” (No pun intended, we think.)
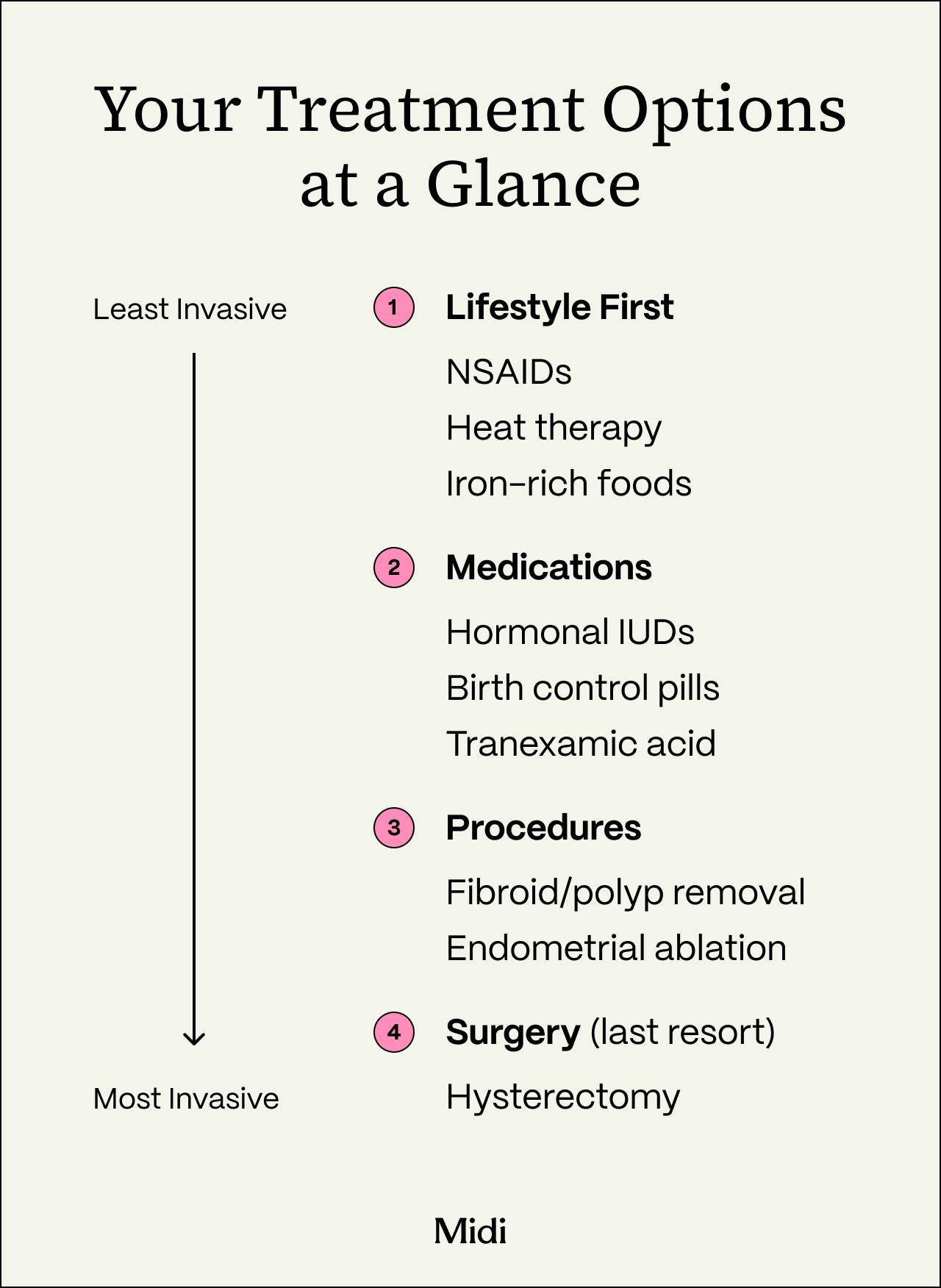
Surgical or Procedural Options
For severe perimenopausal bleeding issues that don’t respond to other treatments, it may be time to explore one of the following options:
- Polyp or fibroid removal: Removing polyps or fibroids (through a procedure called a polypectomy or myomectomy, respectively) can reduce bleeding while leaving the uterus intact if this is the reason for your heavy cycles.
- Endometrial ablation: This procedure thins the uterine lining, which may make periods lighter and more predictable. It’s typically considered only if you are done having children or don’t plan to have any.
- Hysterectomy: A hysterectomy is surgical removal of the uterus. It’s usually reserved for situations where other treatments haven’t helped or heavy bleeding and other symptoms are making it difficult for you to live your life.
Ask your doctor or a Midi clinician to talk you through the pros and cons of these and other options, based on your diagnosis, symptoms, preferences, and health and fertility goals.
When to Contact a Clinician
Heavy perimenopausal bleeding, perimenopausal spotting, and screwy cycles don’t always foreshadow a concerning diagnosis. But some symptoms do require urgent medical attention.
That said, you don’t need to have symptoms on the list below to pursue relief. “Any bleeding that is different from your norm or interferes with your life deserves an explanation, and help is out there,” Dr. Goldman says.
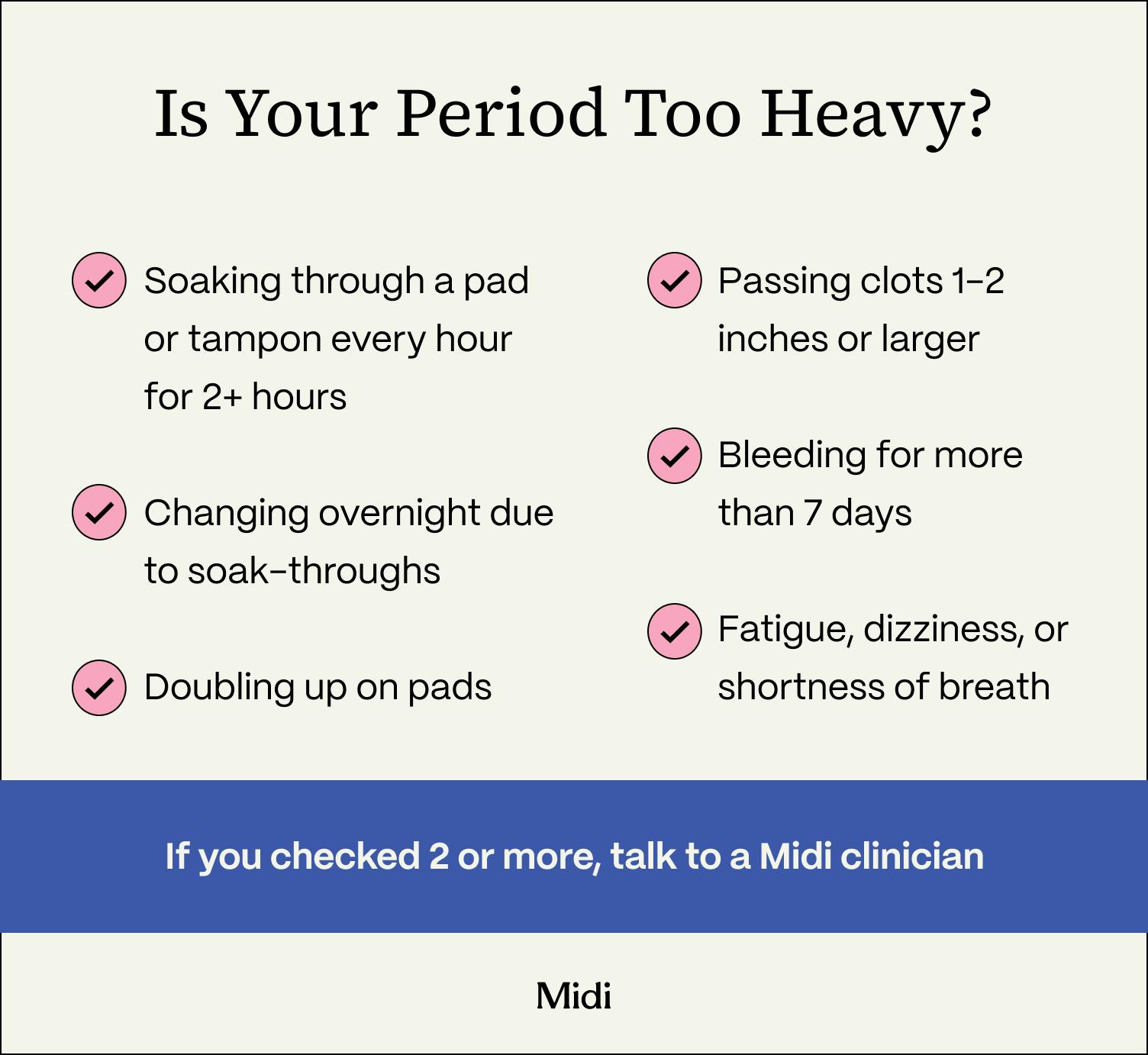
Seek medical care right away if you experience any of the following:
- frequent irregular perimenopausal bleeding—bleeding that doesn’t seem to be stopping after 2 or more weeks or bleeding that seems to be occurring every few days during the month
- a pad or tampon that gets soaked through every hour for 2 or more consecutive hours
- very large blood clots
- heavy bleeding accompanied by dizziness, fainting, shortness of breath, or a racing heartbeat
- severe pelvic pain, especially on one side
- a fever
- any foul-smelling discharge
- a positive pregnancy test with heavy bleeding or one-sided shoulder or pelvic pain
- any postmenopausal bleeding (new onset of bleeding after 12 months without a period)
This list is by no means exhaustive. If anything about your period feels worse or different from your norm, listen to your gut and check in with a healthcare professional or a Midi clinician.
If you’re in perimenopause and craving guidance from clinicians who specialize in women’s midlife health, including perimenopausal bleeding and spotting, consider booking a virtual visit with Midi today. Treatments exist that can help improve your symptoms and ease the physical and mental load of the perimenopausal years.
Key Takeaways
- Irregular, heavier, lighter, or skipped periods are common during perimenopause because estrogen and progesterone fluctuate unpredictably.
- Bleeding that lasts longer than two weeks, happens every few days, or soaks a pad or tampon every hour for two consecutive hours needs medical evaluation.
- Tracking your bleeding for two cycles helps clinicians diagnose the cause and determine the best treatment.
- Abnormal uterine bleeding in midlife may be linked to conditions like fibroids, thyroid disease, PCOS, endometrial hyperplasia, or cancer.
- Effective treatments range from hormonal birth control and HRT to non-hormonal medications and minimally invasive procedures.
Frequently Asked Questions (FAQs)
What are the symptoms of abnormal perimenopausal bleeding?
Symptoms that need medical evaluation include bleeding that lasts more than two weeks, bleeding every few days, soaking through a pad or tampon every hour for two consecutive hours, passing very large blood clots, heavy bleeding with dizziness or shortness of breath, severe one-sided pelvic pain, fever, foul-smelling discharge, or any bleeding after menopause.
When should I see a doctor for perimenopause bleeding?
You should seek care if your bleeding is different from your normal pattern, interferes with your life, or matches any urgent symptoms such as very heavy flow, prolonged bleeding, severe pain, or signs of anemia like fatigue, dizziness, or lightheadedness.
What are the worst symptoms of perimenopause?
In addition to heavy or unpredictable periods, common symptoms include hot flashes, insomnia, mood changes, brain fog, weight gain, breast tenderness, headaches, and worsened PMS symptoms.
Is it normal to bleed constantly during perimenopause?
Cycle changes, heavier periods, spotting, and missed periods are common in perimenopause. However, bleeding that does not stop after two weeks or occurs every few days during the month is not considered normal and should be evaluated by a clinician.
What are the red flags for abnormal uterine bleeding?
Red flags include soaking through a pad or tampon every hour for two hours in a row, very large clots, severe pelvic pain, dizziness, fainting, shortness of breath, fever, foul discharge, or bleeding after 12 months without a period.
If you’re in perimenopause or menopause and want guidance from clinicians who specialize in women’s midlife health, book a virtual visit with Midi today.
Hormonal change is at the root of dozens of symptoms women experience in the years before and after their period stops.
Our trained menopause specialists can help you connect the dots to guide you towards safe, effective solutions.
Whether you need personalized guidance or a prescription routine to tackle symptoms—including brain fog, hot flashes, sleep trouble, mood swings, and weight gain—we’ve got you covered. Learn more here.
Midi’s mission is to revolutionize healthcare for women at midlife, wherever they live and whatever their health story. We believe that starts with education, to help all of us understand our always-changing bodies and health needs. Our core values guide everything we do, including standards that ensure the quality and trustworthiness of our content and editorial processes. We’re committed to providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. For more details on our editorial process, see here.


